The proton Head & Neck (H&N) phantom is IROC Houston's most complex anthropomorphic phantom design for proton therapy, and closely mirrors the IMRT H&N phantom that is used for clinical trial credentialing. The H&N phantom was created with proton-equivalent plastics and an embedded human skull. The phantom contains a horseshoe shaped target, meant to mimic an oropharyngeal tumor, and spinal cord and parotid organs at risk (see Figure 1). The insert also contains TLD and radiochromic film for point and planar dosimetric measurements. The phantom is simulated, planned, and irradiated using the institutions' clinical procedures. Ninety-five percent of the target is to receive 6.6 Gy(RBE). The close configuration of the target and OARs provides a realistic planning challenge for proton TPSs. The criteria for point dose agreement between the TLD and the treatment plan was ±7%, and the criteria for percent of film pixels passing a 7%/4 mm gamma analysis was 85%. The institutions' treatment plans were also assessed for how well they met target and OAR dose constraints.
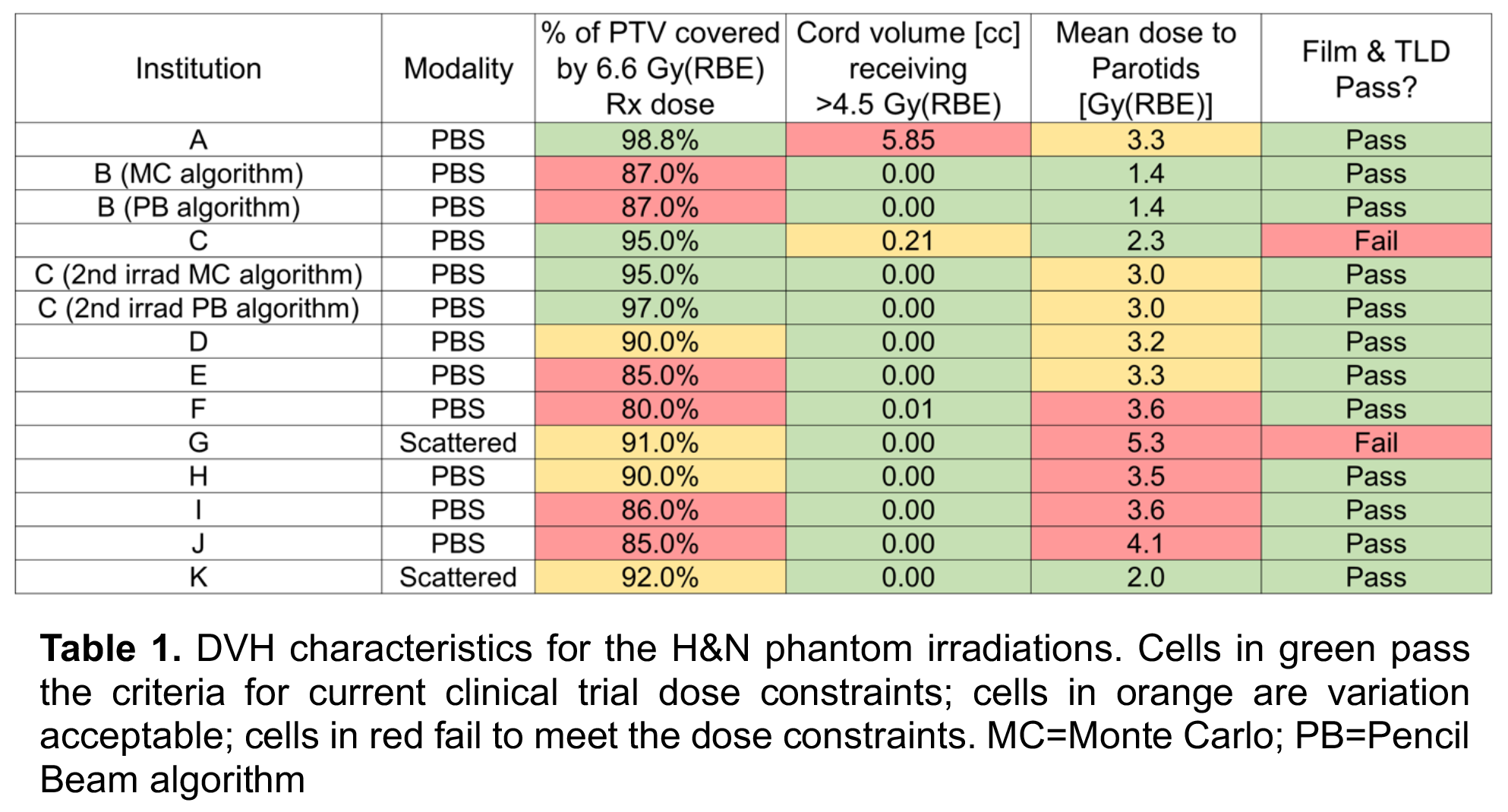
Despite the high phantom pass rate (87%) for the TLD and film measurements, an analysis of clinical dose constraints for the target and OARs showed only 33% of institutions were able to meet all three dose constraint criteria used for clinical trials (see Table 1), and even the institutions that did pass were in the “variation acceptable” category for at least one constraint.
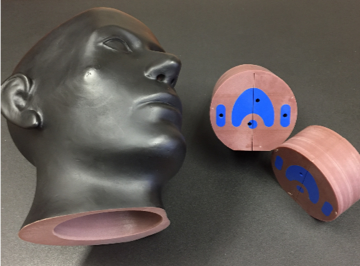 Figure 1. The anthropomorphic proton H&N phantom shown with insert (right). The target, cord, and parotid structures can be seen in blue.
Figure 1. The anthropomorphic proton H&N phantom shown with insert (right). The target, cord, and parotid structures can be seen in blue.
6.6 Gy(RBE) covers ≥95% of the PTV (variation acceptable ≥90%)
Max dose to 0.03 cc ≤4.5 Gy(RBE) (variation acceptable ≤5.0 Gy(RBE))
Mean dose to both parotids ≤2.6 Gy(RBE) (variation acceptable ≤3.3 Gy(RBE))
Many proton centers are able to deliver what they plan to this phantom, however many struggle to meet typical clinical dose constraints for H&N disease. There is a tradeoff between target coverage and OAR sparing in the phantom, just as there is for real patient cases. It may be that some institutions don't try as hard to meet dose constraints on a phantom study as they would with a patient case (despite instructions to treat the phantom like you would a patient). However, these data may encourage clinical trial PIs to add extra scrutiny of proton therapy H&N plans, or they may request that IROC include planning dose constraints as part of the phantom pass/fail criteria. There can be a lot of variability among proton institutions when it comes to target coverage and treatment conformity, largely driven by variations in machine delivery capabilities, but also by clinical experience and treatment planning skill. Clinical trial groups should proceed with caution when adding proton therapy as a modality for H&N trials.
We have noticed that you have an ad blocker enabled which restricts ads served on this site.
Please disable it to continue reading AAPM Newsletter
